
Sabrina Fabi MD, José Raúl Montes MD FACS FACCS, Shino Bay Aguilera DO, Vivian Bucay MD FAAD, Stephanie Manson Brown MBBS MRCS MFPM, Nazanin Ashourian PhD
Cosmetic Laser Dermatology, San Diego, CA
José Raúl Montes Eyes & Facial Rejuvenation, San Juan, Puerto Rico
SHINO BAY Cosmetic Dermatology & Laser Institute, Fort Lauderdale, FL
Bucay Center for Dermatology and Aesthetics, San Antonio,TX
Allergan plc, Marlow, UK
Allergan plc, Madison, NJ
ABSTRACT
Background: Among the growing aesthetic patient population, Hispanic/Latinos represent the largest proportion of non-Caucasians patients. While treatment of Caucasian facial aging patterns are well documented, far less information describes the aesthetic needs of the Hispanic/Latino patient.
Objective: An online study was designed to survey facial aesthetic concerns, treatment priorities, and future treatment considerations among a US-based population of Hispanic/Latino American women.
Materials and Methods: A total of 401 participants ages 30 to 65 years reported their attitudes toward facial aging, current facial conditions, most bothersome facial areas, areas most/least likely to be treated first, awareness of treatment options and their consideration rates, and motives and barriers that factor into consideration of injectable treatments.
Results: Most participants wanted to look good for their age and treatment interests reflected predominant conditions: facial wrinkles, periorbital signs of aging, and uneven skin tone. Most bothersome facial areas included the submental area, periorbital area, and forehead, which were also among the areas most-likely to treat first. The majority of participants would consider injectables. Cost and safety/side effects were cited as frequent concerns.
Conclusion: An understanding of the facial aesthetic concerns and treatment priorities specific to Hispanic/Latino women will enhance the practitioner’s patient-centric treatment approach.
J Drugs Dermatol. 2019;18(7):623-632.
INTRODUCTION
The growing popularity of cosmetic procedures has increased the racial and ethnic diversity of the aesthetic practitioner’s patient population. This growing diversity is reflected by a 52% increase in the total number of Hispanic patients who received cosmetic procedures within the past decade in the USA. Minimally-invasive facial aesthetic treatments are also an increasing trend and accounted for 90% of all procedures performed in the USA in 2017 with neuromodulators and dermal fillers representing mainstay treatment modalities. Among the growing aesthetic patient population, Hispanic/Latinos have represented the largest proportion of non-Caucasian patients (versus African Americans and Asian Americans) receiving neuromodulators and dermal fillers for the last 5 years in a row.
The descriptors “Hispanic” and “Latino” (also known as Mestizo) define an ethnic group which includes individuals of Mexican, Central-to-South American descent, and those of Spanish-Caribbean descent (eg, Cuban, Puerto Rican, and Dominican). Hispanic/Latino Americans are also represented by a range of cultures, languages, and biological ancestry which include Asian, African, European, and native North, Central, and South American. As facial structure and skin type contribute to the characteristic and the progression of facial aging, it must be appreciated that the diversity within the Hispanic/Latino population makes this facial aesthetic patient also potentially the most diverse to treat. The practitioner will need to evaluate and sort out the patient’s predominant phenotype with respect to skin type and baseline facial structure to determine the best treatment approach.
While there is much published on the treatment approaches suitable for non-Hispanic white patients, there are far fewer that address the specific aesthetic needs of the Hispanic/Latino patient. An individual’s racial and ethnic identity also imbues a cultural influence on standards of beauty, attitudes toward appearance, and priorities in the management of facial aging. For the culturally-competent practitioner, an awareness of not only the structural and cutaneous signs of aging but also the patient’s attitudes toward aging are integral in a patient-centric treatment plan.
The current study aimed to survey the facial aesthetic concerns and treatment priorities among a population of Hispanic/Latino American women who were aesthetically-oriented yet naïve to facial injectable treatment use. The data encompassed: 1) attitudes toward signs of facial aging and current facial conditions; 2) facial areas that are most bothersome; 3) facial areas most/ least likely considered a priority in a future aesthetic treatment plan; 4) awareness of available aesthetic treatments and their consideration rates, and 5) motives and barriers factoring into consideration of injectable treatments.The data presented here is a subset of a larger study which consisted of 1205 women and also included African American and Asian American participants.
METHODS
Participants and Study Design
Participants were recruited through online river sampling (banner ads, pop-up ads, instant capture promotions) by the
Lieberman Research Worldwide (LRW) agency between March and April 2016. Primary inclusion criteria were: 1) females ages 30 to 65 years old living in the USA; 2) aesthetically-oriented, qualified by level of agreement on an aesthetic orientation screening questionnaire; 3) household annual income >$50,000 with some discretionary spending flexibility ; 4) naïve to facial injectable treatments; 5) aware of BOTOX® Cosmetic; and 6) considering a medical facial aesthetic treatment within the next 2 years.
Participants identified their ethnic background as one of the following: Mexican, Mexican American, Puerto Rican, Cuban, or “Other Spanish, Hispanic, or Latino”. A questionnaire adapted from the Skin Cancer Foundation website was used to categorize participants by Fitzpatrick Skin Phototype (FSP) I through VI. The questionnaire took into account eye color, natural hair color, skin color (non-exposed areas, presence/ absence of freckles (non-exposed areas), and skin response to ultraviolet radiation (UVR), including the susceptibility of facial and body skin to burn or turn brown (tan) following exposure. Participants also identified their pigmentary characteristics by selecting a color most representative of their natural skin tone from a range of 11 skin codes (colors).
MEASURES AND ANALYSIS
Attitudes Toward Facial Aesthetics and Existing Facial Concerns Questionnaire
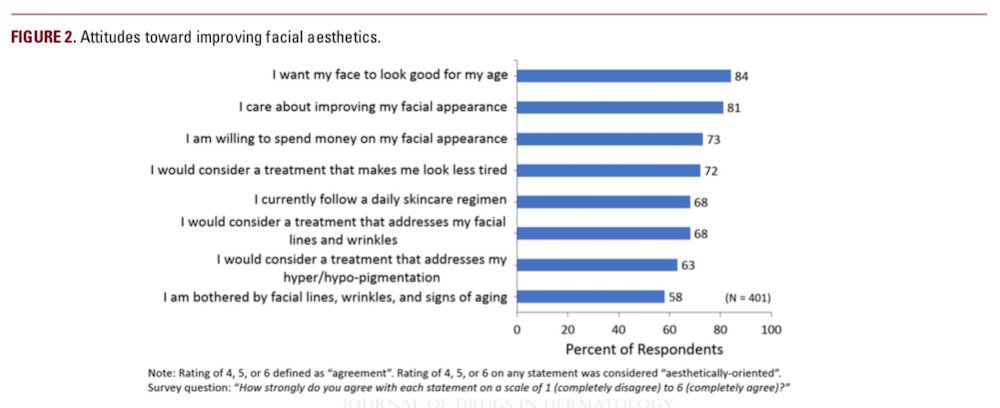
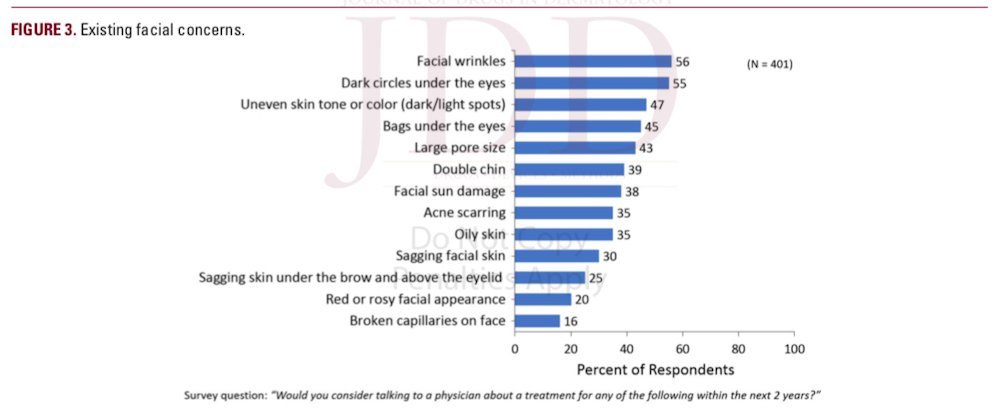
Attitudes toward improving facial aesthetics were assessed by the aesthetic orientation screening questionnaire which included a list of options paired with the question “How strongly do you agree with each statement on a scale of 1 (completely disagree) to 6 (completely agree)?” Existing concerns were identified from a list of options paired with the following question: “Would you consider talking to a physician about a treatment for any of the following within the next 2 years?”
Most Bothersome Facial Areas and Treatment Priorities Questionnaires
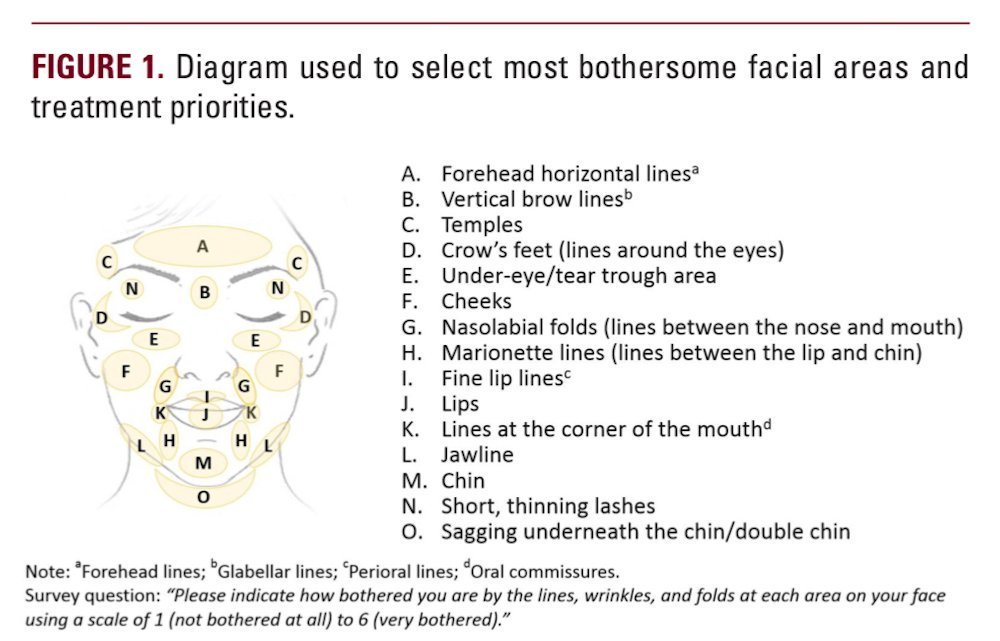
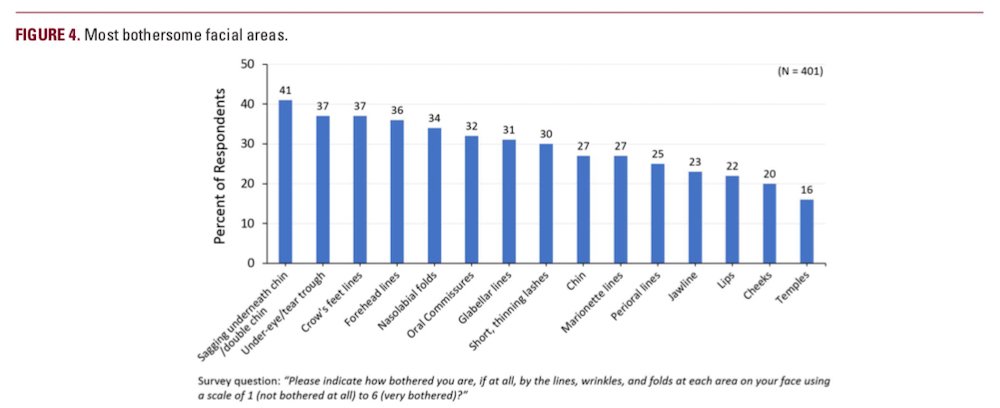
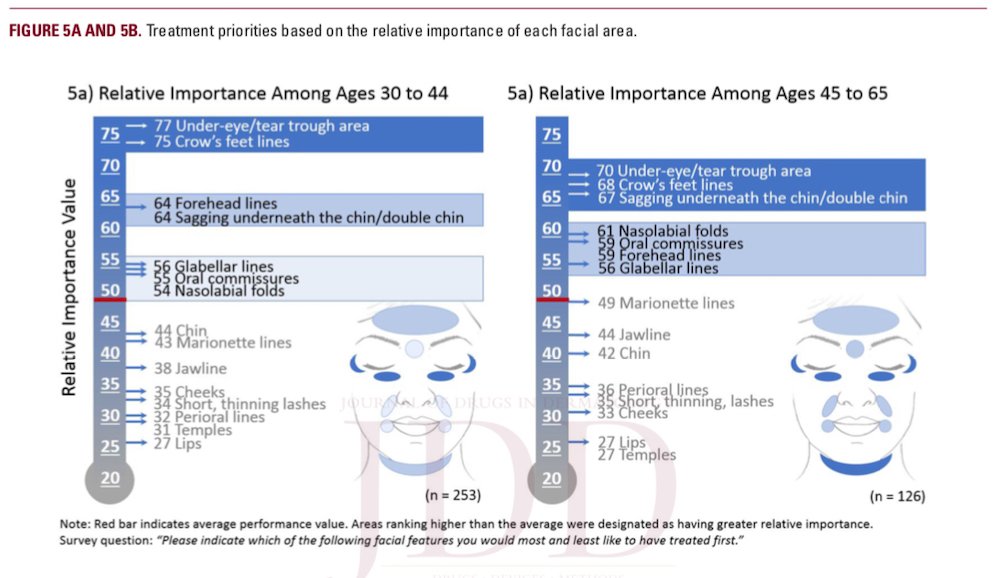
A 15-point facial diagram and a 6-point Likert scale (1, “not at all bothered” to 6, “very bothered”) were used to assess how bothersome each area was if at all (Figure 1). A Maximum Difference (MaxDiff) ranking methodology, also referred to as “Best/Worst scaling” was then used to generate a rank order of each area as it relates to treatment priority. Nine different iterations of the facial diagram were shown, each consisting of 3 facial areas at a time until all 15 features were presented. With each iteration, 1 area was selected as the “most likely to be treated first” and 1 area as the “least likely to be treated first”. MaxDiff ranking scores were represented by a “relative importance value”. An average ranking of importance was established among all areas combined. Areas ranking above average represented greater importance and priority relative to those areas ranking close to or below the average.
Awareness of Aesthetic Procedures and Future Treatment Considerations Questionnaires
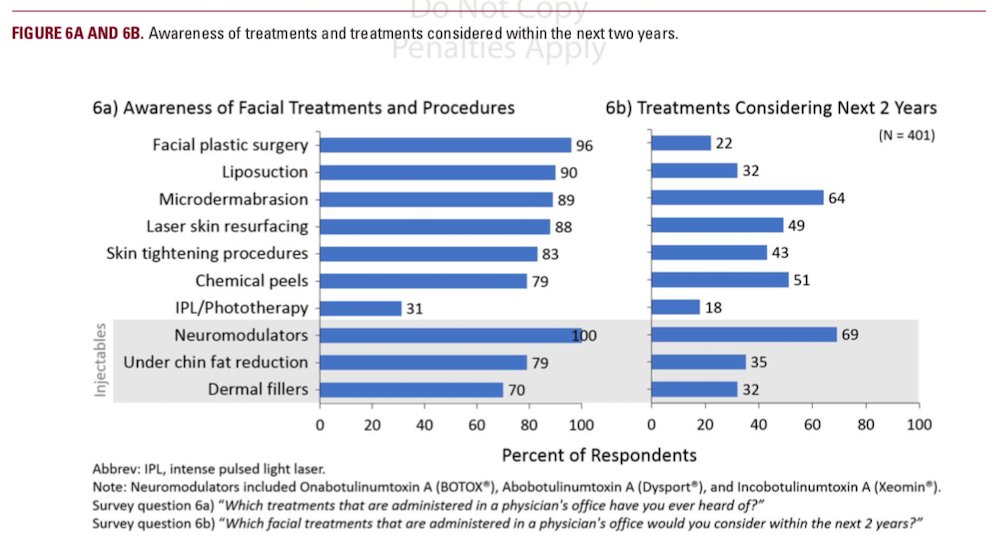
Treatment procedure awareness and future treatment considerations were identified from a list of options paired with the questions: “Which treatments that are administered in a physician’s office have you ever heard of?” and “Which facial treatments that are administered in a physician’s office would you consider within the next 2 years?”
Motives and Barriers Impacting Consideration Rate of In- jectable Treatment Questionnaires
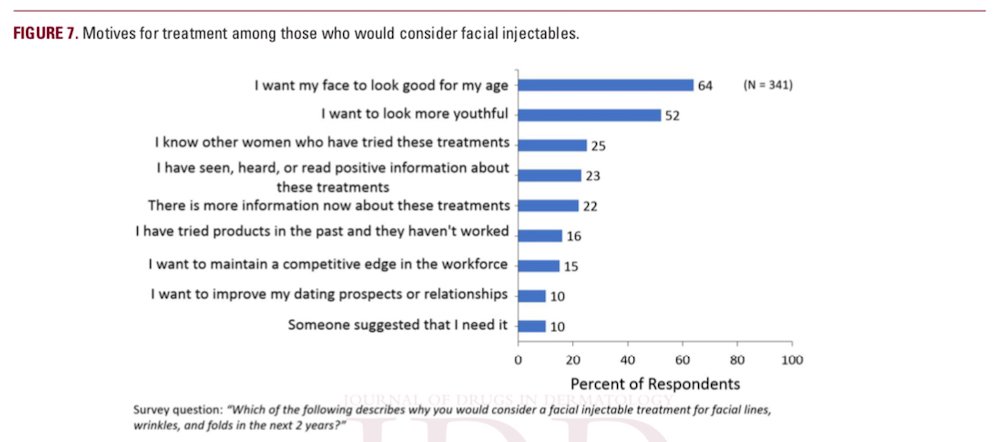
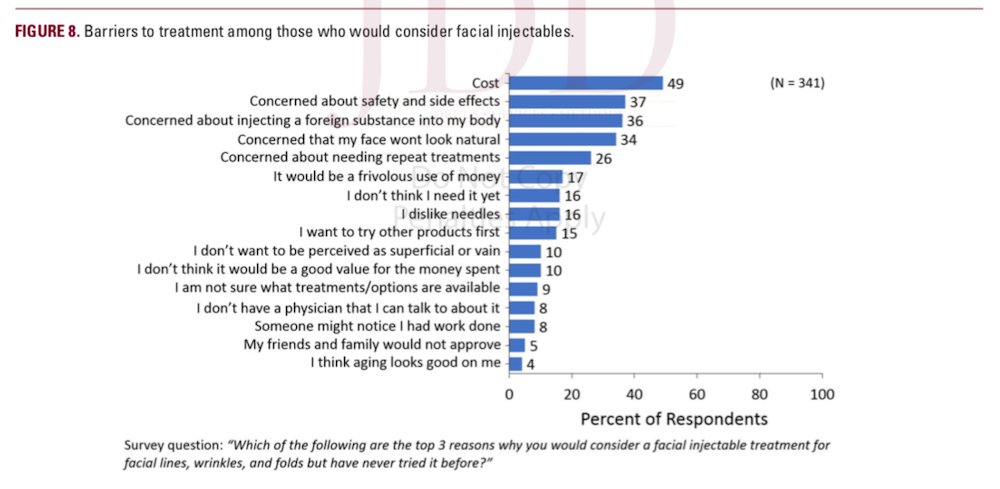
Motives and barriers were identified from a list of options paired with the questions: “Which of the following describes why you would consider a facial injectable treatment for facial lines, wrinkles, and folds in the next 2 years?” and “Which of the following are the top 3 reasons why you would consider a facial injectable treatment for facial lines, wrinkles, and folds but have never tried it before?”
Data Analysis
Max Diff analyses and analysis for correlation between bothersome facial areas and their treatment priorities were conducted by the LRW agency and presented descriptively by percent or by average.
RESULTS
Participants
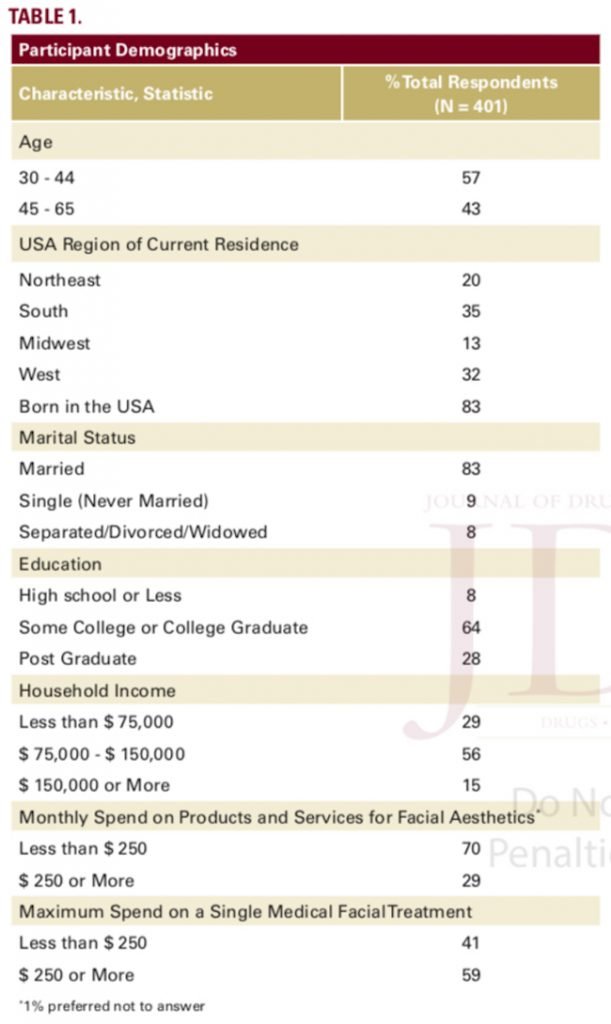
The majority of the 401 participants included in the study were 30 to 44 years old (57%), born in the USA (83%), married (83%), with household income > $75,000 (71%), an average spending of < $250/month on facial aesthetic products/services (70%), and had previously spent ≥ $250 on a single medical facial treatment (59%; Table 1). The majority were categorized as FSP III or IV (71%) and a large proportion (46%) self-identified with a Mexican ethnic background (Table 2).
Attitudes Toward Improving Facial Aesthetics and Existing Facial Concerns
Most participants agreed with the statement that they wanted their face to look good for their age (84%). A large proportion was interested in treatments that could make them look less tired (72%), and that would address facial lines/wrinkles/ signs of aging (68%) as well as hyper/hypo-pigmentation (63%) (Figure 2). Facial wrinkles (56%), dark under-eye circles (55%), uneven skin tone/color (47%), and bags under the eyes (45%) were among the most frequently-reported conditions (Figure 3).
Most Bothersome Facial Areas
The most bothersome areas included sagging underneath the chin/double chin (41%), under-eye/tear trough area (37%), crow’s feet lines (CFLs) (37%), and forehead lines (FHLs) (36%). These were followed by glabellar lines (GLs) (31%) and areas of the mid-to-lower face, including nasolabial folds (NLFs) (34%), oral commissures (OCs) (32%), chin (27%), and marionette lines (MLs) (27%; Figure 4). Perioral lines (25%), jawline (23%), lips (22%), cheeks (20%), and temples (16%) were the least bother- some areas.
Treatment Priorities
The treatment priorities of each facial area (represented by relative importance scores) ranged from 27 to 77 with treatment priorities tending to correlate with bothersome facial areas (R2 =.81, data not shown). In younger participants (ages 30 to 44), areas of the upper face had the highest priorities and included the under-eye/tear trough area (77) and CFLs (75; Figure 5a). Other areas of high importance were FHLs (64), sagging underneath the chin/double chin (64), GLs (56), OCs (55), and NLFs (54). Mid-to-lower facial areas such as chin (44), MLs (43), jawline (38), and cheeks (35) were lower priorities, and perioral lines (32), temples (31), and lips (27) were the least likely to be prioritized for treatment.
For the older participants (ages 45 to 65), under-eye/tear trough area (70) and CFLs (68) remained a top priority but sagging underneath the chin/double chin had increased importance (67; Figure 5b).
Subsequent priorities were NLFs (61), OCs (59), FHLs (59), and GLs (56), followed by MLs (49), jawline (44), and chin (42). Mid- to-lower facial areas such as perioral lines (36) and cheeks (33) were lower priorities, and lips (27) and temples (27) were the lowest priorities.
Awareness of Treatments Options and Future Treatment
Consideration Rates
Most participants were aware of the treatments or procedures used to enhance skin quality such as microdermabrasion (89%), laser skin resurfacing (88%), skin tightening procedures (83%), and chemical peels (79%; Figure 6a), and high consideration rates were observed for those treatments within the next 2 years (43 – 64%; Figure 6b). Furthermore, all were aware of neuromodulators (100%), most were aware of under chin fat reduction (79%) and dermal fillers (70%) products, with 69%, 32%, and 35% consideration rates, respectively.
Motives and Barriers Impacting Consideration Rate of Injectable Treatments
Among the 84% (341/401) who would consider an injectable treatment, the most common motives were wanting their face to look good for their age (64%) and to look more youthful (52%; Figure 7). Interestingly, a much smaller proportion agreed with wanting to maintain a competitive edge in the workforce (15%) and to improve dating prospects or relationship prospects (10%). The top 3 most common barriers cited for not having tried injectable treatments yet were cost (49%), concerns about safety and side effects (37%), and concerns about injecting a foreign substance into their body (36%; Figure 8). In alignment with this, among the 16% of participants who would not consider injectables, the primary barriers included concerns about safety and side effects (66%), injecting a foreign substance into their body (52%), and concern that their face would not look natural (34%) (data not shown).
DISCUSSION
The rate of onset, severity, and pattern of facial aging is influenced by race and ethnicity, while the motives that prompt an individual to seek treatment may be based more on social and cultural ideals of beauty and attitudes about improving their facial aesthetics. In this survey of 401 Hispanic/Latino American women aged 30 to 65, the predominant aesthetic concerns and goals were reported, which may help familiarize practitioners with this patient population and help guide relevant treatment plans.
Attitudes Toward Improving Facial Aesthetics
Participant attitudes about facial aesthetic treatments suggested that attitudes and treatment interests may stem from current skin and facial conditions, which are also influenced by an individual’s ethnic background. A high proportion of responders considered treatments that would make them look less tired (72%) and address facial wrinkles and lines (68%) and hyper/ hypo-pigmentation (63%); correspondingly, a majority also reported having facial wrinkles (56%), dark circles under the eyes (55%), uneven skin tone/color (47%), and bags under eyes (45%). Although the greater melanin content in more darkly pigmented skin types affords some protection against the immediate effects of UV exposure (eg, sun burn), photodamage still occurs and results in pigmentary changes (eg, freckling, solar lentigo, and melasma) and increases an individual’s risk factor for post- inflammatory hyperpigmentation (PIH) following inflammation or injury. Melasma and hyperpigmentation are believed to occur more frequently in Hispanic and Latino ethnicities, with as many as half of all Mexican women reporting melasma associated with pregnancy.
Most Bothersome Facial Areas and Treatment Priorities
Bothersome facial areas correlated somewhat with treatment priorities (R2 =.81, data not shown), and any discrepancy (ie, lower importance for short, thinning lashes) might represent areas more easily enhanced by the application of cosmetics versus those that are not. The most bothersome facial areas reported by all were sagging underneath the chin/double chin, under-eye/ tear trough, CFLs, and FHLs. While these all translated to areas with high treatment priority, differences between the younger and older age groups were observable. Among the more advanced age group (45 to 65-year-olds) sagging underneath the chin/double chin and areas of the lower face (OCs and NLFs) increased in relative importance in comparison to the younger age group (30 to 44-year-olds). This result is expected since increasing midface ptosis, which accompanies facial aging, can exacerbate grooves and folds in the lower face and displace the importance assigned to areas of the upper face (under-eye/ tear trough, CFLs, and FHLs) at a younger age. Also aligned with that reasoning is the change in the importance of the marionette lines (MLs) and the jawline, which were scored as lower priorities by the younger group but increased in importance in the older group.
Overall, areas of the upper face (under-eye/tear trough and CFLs) were assigned greater relative importance than the lower face. Although this is expected as areas of the upper face tend to reveal more of the initial signs of aging, it is important to note that participants were not given the option to differentiate between under-eye and tear trough.The cause of dark under-eye circles are multifactorial and could be attributable to periocular inflammation, blood stasis, uneven pigmentation, or may be the result of shadowing caused by tear trough deformity. With aging, the orbital bone resorption, loss of midface volume, and increasing skin laxity can be associated with increased severity of tear troughs, which are characterized by a concavity separating the lower eyelid from the cheek. Therefore, this may imply that dark circles under the eyes is a common phenomenon in the Hispanic/Latino population, and may represent key aesthetic concerns for this patient population.
Mestizo or Hispanic individuals with Native American origins share greater craniofacial similarity with Asians than with whites. In this light, it should be considered that some Hispanic/Latino patients may also share some of the facial aging patterns observed with the Asian ethnicities. While both Hispanic and Asian facial shape can be characterized as broad (wide bizygomatic and bigonial distance) with heavier malar fat pads, certain Asian ethnicities also tend to have less anteromedial midface projection, which may contribute to the gravitational descent that exposes the tear trough. In another similarity with Asians, aging of the Mestizo face may include an increase in the forehead-glabella supraorbital prominence contributing to superior concavity and shadowing of the forehead. Orbital bone resorption also contributes to descent of the lateral third of the eye brow, and for Mestizo individuals, heaviness of the brow and hooding of the eyelids may also be more pronounced due to a thicker, heavier skin type.
The high importance level and priority assigned to sagging underneath the chin/double chin in both older and younger
participants may reflect gravity-induced changes associated with a heavier, thicker skin type in the Hispanic/Latino population. This is in contrast to descent due to increased skin laxity accompanied by jowling that is observed more often in Caucasians. Other anatomical contributors may include a recessed chin position, a facial characteristic observed more often in the Asian and Hispanic/Latino ethnicities that may exacerbate the appearance of the submental fat. It is, however, important to note that participants were not able to differentiate between “sagging underneath the chin” and “double chin.” Body mass index (BMI) can contribute more significantly to the appearance of submental fullness than skin laxity or sagging. As BMI was not measured in this study, we cannot determine if the high prevalence of sagging underneath the chin/double chin in the Hispanic/Latino population may be a consequence of differences in the BMI in this group.
Consideration Rates for Future Treatments Including Injectables
Although there appeared to be a high awareness of injectable treatments involving under chin fat reduction and dermal fillers, they corresponded with lower consideration rates than other minimally-invasive treatments such as microdermabrasion, chemical peels, and laser skin resurfacing. Interestingly, although underneath the chin area was a high priority and 79% of participants were aware of the injectable treatments available for this area, only 35% would consider having this treatment. This observation may reflect a gap in patient knowledge. There was a higher consideration rate for neuromodulators compared with all other minimally-invasive treatment options. This observation agrees with previous studies highlighting the aesthetic preferences of Hispanic/Latino patients and is exemplified by the fact that this population makes up the greatest proportion of ethnic minority patients receiving treatment with neuromodulators.
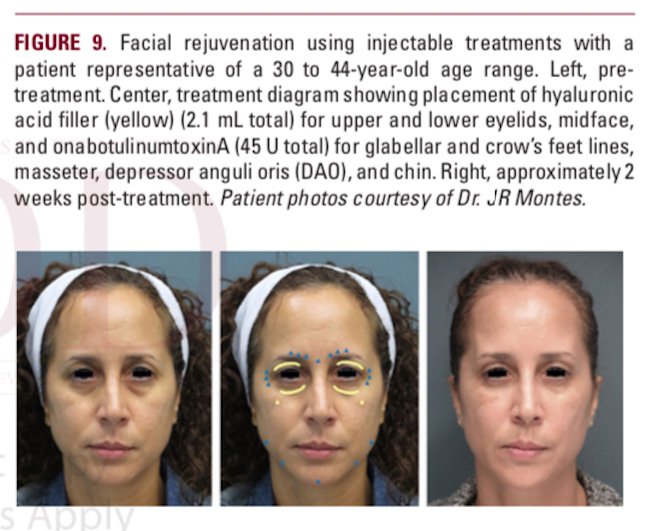
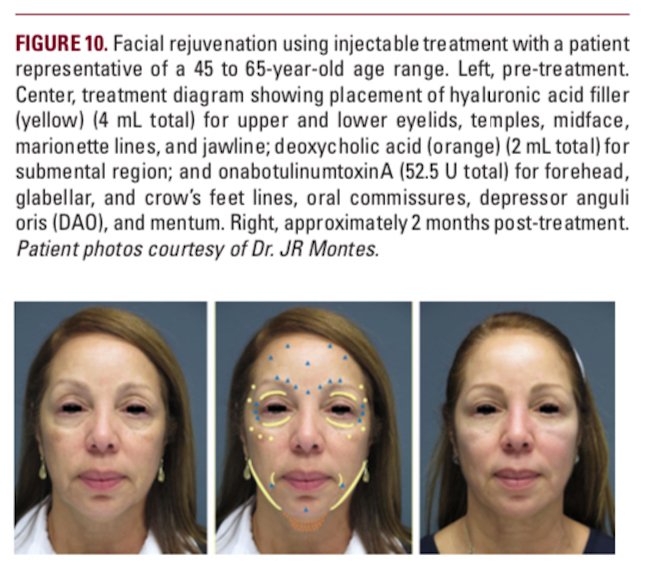
The strengths of this study include a large participant population, a cross-sectional design, and the use of MaxDiff methodology to minimize scale bias, as compare to using paired comparisons. The data collected and presented here characterizes the priorities and treatment awareness among a diverse population of Hispanic/Latino Americans naïve to facial injectable use and helps clinicians to understand this population and to plan treatments accordingly. Two case examples of Hispanic/Latino patients treated by the authors are presented in Figure 9 and Figure 10.
CONCLUSIONS
Hispanic/Latino Americans are a growing patient population for aesthetic practitioners. As much of the literature pertaining to facial aesthetic rejuvenation is focused on Caucasian women, there is a need to explore the facial aging process among Hispanic/Latino women and identify the attitudes that factor into their consideration of the different treatments. Compared to other racial/ethnic groups, Hispanic/Latino women comprise a diverse racial and ethnic background with signs of facial aging that may share common patterns and characteristic of other racial/ethnic groups, but the practitioner will need to keenly identify them.
This survey highlighted key aesthetic concerns common among the Hispanic/Latino American women and revealed the most bothersome areas for this population as the under-eye/tear trough area, CFLs, FHLs, and the submental area. With advancing age, priorities shifted slightly from upper facial areas to include more of the mid and lower facial areas. In addition, the discrepancy between the high level of aesthetic concern for underneath the chin area and low consideration rate for the injectable treatments for this suggest there may be opportuni- ties to educate patients regarding available treatments that may help them achieve aesthetic goals.
Among participants who would not consider injectables, the main reasons cited were concerns about safety/side effects, concerns about putting a foreign substance into their body, and concern that their face will not look natural. Educating and counseling patients on these barriers may increase patient acceptability of a broader range of treatment options and comfort them in knowing there is a reinforcement on “naturalness” in medical aesthetic treatments. By lessening the barriers to injectables, patients may ultimately achieve a more impactful and longer lasting treatment results. Also, discussing treatment strategies that address existing pigmentary issues and minimize the risk of PIH may help strengthen the patient-practitioner bond.
With the observations presented here, this study hopes to contribute to a first step in providing practitioners with a more patient-centric and culturally-competent approach to their treatment of Hispanic/Latino facial aesthetic patients.
DISCLOSURES
S Fabi serves as a consultant, researcher, and advisory board member for Allergan plc. JR Montes serves as a speaker and trainer for Allergan plc. SB Aguilera serves as a speaker and trainer for Allergan plc. V Bucay serves as a speaker and consultant for Allergan plc. S Manson Brown and N Ashourian are employees of Allergan plc and may own stock/options in the company. The opinions expressed in this article are those of the authors. The authors received no honoraria related to the development of this article. This study was funded by Allergan, Inc. Writing and editorial support for this article was provided by Erika von Grote, PhD, Allergan plc, Irvine, CA.The authors would like to thank GarrettT. Shumate of Allergan plc for his invaluable assistance in the interpretation of data and in the development of this manuscript.
REFERENCES
1. 2008 ASAPS Statistics: Complete Plastic Surgery Statistics Report. American Society for Aesthetic Plastic Surgery. Available from: http://www.sur- gery.org/sites/default/files/2008stats.pdf. Accessed October 2018.
2. 2017 ASAPS Statistics: Complete Plastic Surgery Statistics Report. American Society for Aesthetic Plastic Surgery. Available from: http://www.surgery. org/sites/default/files/2017stats.pdf. Accessed October 2018.
3. https://www.plasticsurgery.org/news/plastic-surgery-statistics. Accessed October 2018.
4. Bertoni B, Budowle B, Sans M, Barton SA, et al. Admixture in Hispanics: distribution of ancestral population contributions in the continental United States. Hum. Biol. 2003;75:1-11.
5. Talakoub L, Wesley NO. Differences in perceptions of beauty and cosmetic procedures performed in ethnic patients. Semin Cutan Med Surg. 2009;28(2):115-129.
6. Davis EC, Callender VD. Aesthetic dermatology for aging ethnic skin. Dermatol Surg. 2011;37(7):901-917.
7. Alexis AF, Alam M. Racial and ethnic differences in skin aging: implications for treatment with soft tissue fillers. J Drugs Dermatol. 2012;11(8):s30-s32; discussion s2.
8. Vashi NA, de Castro Maymone MB, Kundu RV. Aging differences in ethnic skin. J Clin Aesthet Dermatol. 2016;9(1):31-38.
9. Cobo R. Trends in facial plastic surgery in Latin America. Facial Plast Surg. 2013;29 (3):149-53.
10. Broer PN, Juran S, Liu YJ, Weichman K, et al. The impact of geographic, ethnic, and demographic dynamics on the perception of beauty. J Craniofac Surg. 2014;25(2):e157-161.
11. Montes JR. Ethnic and Gender Considerations in the Use of Facial Injectables: Latino Patients. Plast Reconstr Surg. 2015;136(5 Suppl):32S-39S.
12. Boyd C, Chui A, Montes JR, Narurkar V, et al. Differential facial aesthetic treatment considerations for skin of color populations: African American, Asian and Hispanic. Poster presented at: The Skin of Color Seminar Series; May, 2018; New York, NY.
13. Fitzpatrick TB. The validity and practicality of sun reactive skin types I-VI. Arch Dermatol. 1988;124:869-871.
14. https://blog.skincancer.org/2018/09/13/are-you-at-risk-for-skin-cancer/Assessed February 2019.
15. Ho BK, Robinson JK. Color bar tool for skin type self-identification: A crosssectional study. J Am Acad Dermatol. 2015;73(2):312-3.e1.
16. The MaxDiff System Technical Paper, Version 8. Sawtooth Software 2015;Available at: URL: http://www.sawtoothsoftware.com/support/technical-papers/maxdiff-best-worst-scaling/maxdiff-technical-paper-2013.
17. Del Bino S, Duval C, Bernerd F. Clinical and biological characterization of skin pigmentation diversity and its consequences on UV impact. Int J Mol Sci. 2018;19(9). pii: E2668.
18. de Rigal J, Des Mazis I, Diridollou S, Querleux B, et al. The effect of age on skin color and color heterogeneity in four ethnic groups. Skin Res Technol. 2010;16(2):168-178.
19. Sanchez MR. Cutaneous diseases in Latinos. Dermatol Clin. 2003; 21:689-697.
20. Friedmann DP, Goldman MP. Dark circles: etiology and management options. Clin Plast Surg. 2015;42(1):33-50.
21. Matsui MS, Schalka S, Vanderover G, Fthenakis CG, et al. Physiological and lifestyle factors contributing to risk and severity of peri-orbital dark circles in the Brazilian population. An Bras Dermatol. 2015;90(4):494-503.
22. Kahn DM, Shaw RB Jr. Aging of the bony orbit: a three-dimensional computed tomographic study. Aesthet Surg J. 2008;28(3):258-264.
23. Glaser DA, Lambros V, Kolodziejczyk J, et al. Relationship between midface volume deficits and the appearance of tear troughs and nasolabial folds. Dermatol Surg. 2018;44(12):1547-1554.
24. Dudzik B, Jantz RL. Misclassifications of Hispanics Using Fordisc 3.1: comparing cranial morphology in Asian and Hispanic populations. J Forensic Sci. 2016;61(5):1311-1318.
25. Oranges CM, Gohritz A, Haug M, Harder Y, Schaefer DJ. Universal and ethnic-specific considerations on facial rejuvenation: where do you inject your